
Core Principles

The Low Back System
How to deal with back and other pains
A few years ago I did something to my back while lifting something heavy and finally joined the ranks of the several million or so people who experience low back pain (box 1.). Having believed myself immune to this condition, and having dealt in a professional capacity with scores of people with back pain, it was instructive to finally experience it myself. I had the typical symptoms: a feeling of intense tightness in my lumbar region which I could somehow never stretch out; some muscle in my right buttock which seemed permanently locked, a catching pain that would have me limping to my morning coffee, a distressing electric pain shooting down the back of my legs and, as time wore on, a growing sense of frustration and misery. No matter how much I stretched, massaged, rolled or exercised, I just could not break this beast.
It took around a year before I turned a corner and, quite quickly, managed to unlock the back pain. It felt miraculous when the pain finally went away. I cannot say for certain if the particular exercises I chose were what did the trick - perhaps the underlying cause/s would have resolved regardless - but the resolution of the pain coincided almost exactly within a few weeks of me finding a particular series of exercises. At the risk of disappointing the reader early on, I won’t go into the exact details of the workout I chose (I’ll include a link presently) because an important point I want to stress is that every body is different and therefore every back pain is different and so what what works for you will be different from me. However there are a few common principles which will more or less apply to anyone regardless of physique or fitness.
Before this there is one more aspect of my ‘back pain story’ worth mentioning. For a long time I was searching for the cause of the pain. I believed that somewhere in my back was some culprit that, if only I could only find it, I could cure it. I imagined some particular spot - perhaps an inflamed nerve root, a herniated disc, a locked piriformis muscle etc. - that if I could pin down, I could treat.
This search, of course, proved fruitless. The fugitive pain would shift locations day to day, always one step ahead of me. Part of my ‘breakthrough’ (though there was no light-bulb moment, just a slow realisation) was when I widened the scope of my enquiries: rather than try to find a culprit, why not approach the whole back as a system? Maybe the pain did not originate where I felt it most. Perhaps if I worked on other areas away from the pain like the hips, legs, etc, then the imbalances that were perpetuating the pain would resolve… and so it transpired.
Box 1. The Burden of Low Back Pain (LBP)
Up to 84% gen pop will experience LBP at some point in their lives
6-8% cases can become chronic
One-in-five cases result in sick leave and represent 30% sick leaves lasting over 6 months
Leading cause of work exclusion in under 45-year olds
(Note above refers to non-specific non-radiating pain low back pain)
'Chronic Low Back Pain: A Narrative Review of Recent International Guidelines for Diagnosis and Conservative Treatment' Journal of Clinical Medicine 2023
An Image Problem
We often find it easier to see problems in terms of their isolated parts. Moreover we often imagine these parts as static things. We might even give them a character or personality, or ascribe some value such as good or evil to them. What is less obvious are the relationships between the many parts of any given problem, and the fact that each of these parts is changing over time. The musculoskeletal system is a classic example of this: A change of position of one part of it will affect movement in a seemingly distant part.
It is hard to appreciate the dynamic nature of our bodies with static words and anatomical images. In fact, using certain words or images to describe a problem can significantly worsen it due to their psychological effects. So for instance ‘slipped disc’ brings to mind the image of a disc ‘slipping’ from between the vertebral bones like a bar of soap, straight towards the spinal cord. This is nowhere near the reality - at worse a portion of the rubbery disc can herniate through the fibrous ring surrounding it and press against the tough sheath covering the spinal cord but only rarely do they actively pinch a nerve.
Likewise phrases like ‘wear and tear’ or, even worse, ‘crumbling spine’ in no way correspond to how bones are continually remodelling. I often hear people talk about ‘ageing’ as a cause for pain but even this word is dubious. This isn’t to say that getting older is not a biological reality, rather that the loss of independence and agility we ascribe to it are often more likely to be due to de-conditioning, or more accurately loss of access to activity that maintains an optimal condition.
Another complication is that when we experience pain in a particular part of our bodies we naturally focus on that part. In acute situations this is fair enough: in the case of a broken bone for instance, it is sensible firstly to fix the bone and not worry about the bigger picture. However this is less the case in more chronic pain, where the pain may not actually be in any spot at all.
It is entirely natural to try and find the cause of pain. However, in a complex system like the back, the search can often be futile, if not counterproductive. If, as research suggests, around two-thirds of adults have some sort of ‘abnormal’ disc anyway, then any scan for back pain which ‘reveals’ an abnormal disc isn’t especially useful. (box 2.)
Box 2. Why searching for a cause isn’t generally helpful (and can be harmful)
No published data has found a specific history or examination that would indicate structures causing pain
Only one guideline (from France in 2021) recommend MRI in chronic low back pain lasting >3 months
American College of Occupational and Environmental Medicine clearly concluded that diagnostic testing is not indicated for the majority of people with low back pain.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9964474/pdf/jcm-12-01685.pdf
Should you get an MRI?
MRIs were done on 98 non-symptomatic subjects:
Only 36% had normal disks at all levels.
52% had bulge at at least one level
27% had protrusion and 1% disc extrusion
'Magnetic Resonance Imaging of the Lumbar Spine in People without Back Pain' NEJM 1994
When to be concerned
As the aim of this article is to hopefully remove a lot of the worry and mystery around back pain, we ought to mention those features which would require medical attention. A recent study showed that a very small proportion - around 1% - of people with low back pain may have a serious issue, such as fracture, malignancy, infection, spondyloarthritis or cauda equina syndrome. The prevalance is around 2.4% for fracture, 0.7% infections, 0.5% malignancy and 0.3% cauda equina - though bear in mind this all depends on the age of the patient and where they present (an emergency doctor will see more serious issues than a family doctor).
‘Red flags’ are not actually that reliable, but for what they are worth they include features like nocturnal pain, associated night sweats and/or weight loss, sudden urinary retention and faecal incontinence and worsening pain in the upper back (thorax). Of course, if in doubt, just get it checked out.
'Recent highlights in low back pain research' Journal of Physiotherapy (Australian Physiotherapy Association) January 2023
What is the Goal of the Lower Back System?
A systems approach zooms out from any specific cause and looks more at processes like relationships and functions or goals. So, what is the function of the low back system (LBS)? In theory you can pick any answer within reason, but we’ll say that the goal of the LBS is to maintain a balance between movement and stability in order to carry out activity.
You may notice that movement and stability are actually conflicting aims: an entirely stable system won’t move, and a completely free system won’t be stable. As with so much in biology, the organism maintains a dynamic balance between often conflicting forces. The spine provides a neat example of this. (fig 1.)
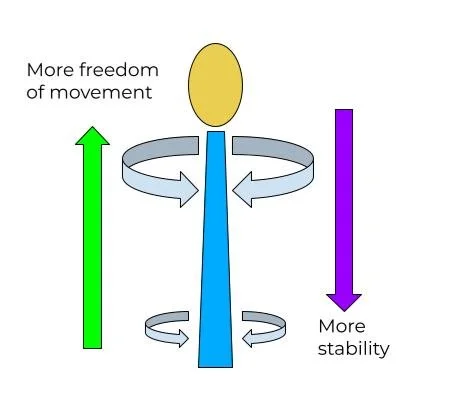
Fig 1. The further up the spine we go, the greater the mobility including rotation, bending forward and back, and side to side.
Rotation Vs Twisting
We can glean a couple of practical lessons from this. They can be summed up under the principle of ‘heavy to stable, light to mobile’. What this means is that, in order to reduce strain, we should avoid placing heavy loads on parts of the spine less capable of bearing them. Likewise if something has evolved to move a certain way then why not make use of that? For example when turning our heads, we often twist at the neck (especially if we’re sitting), which places strain on the cervical spine and soft tissue of the neck, which can lead to neck pain and headaches. To avoid this we use the entirety of the thoracic spine, which is evolved to rotate quite freely. (fig 2.)
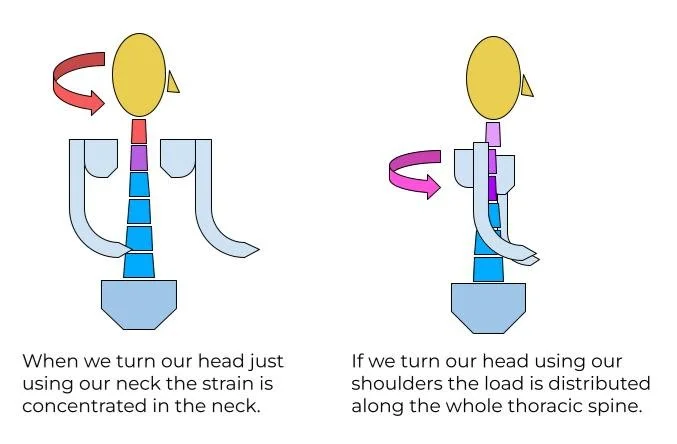
Fig 2. To appreciate this, try the flowing exercise: slowly turn your head from side to side as you would normally, and note any tension. Now place your hands on your cheeks, tuck in your elbows and repeat, again turning slowly from one side to the other. Finally take your hands down and repeat the motion. Do you find the motion easier? Are you using your shoulders and rotating the upper spine more, rather than just twisting your neck?
Hips = Fulcrum
Similarly most of us know that when picking up heavy loads we shouldn’t stoop. Why? Because stooping distributes the load along the less stable, more mobile upper spine. We also end up mainly using our lumbar muscles to lift the load - a recipe for back injury. On the other hand by keeping the lower spine solid, using the lumbar muscles as a brace, hinging at the hip and using our glutes to lever up the load we are using the strongest muscles in the most stable configuration. Interestingly by bracing the core and holding our breath in we increase intra-abdominal pressure which significantly increases the stability of our lower back.
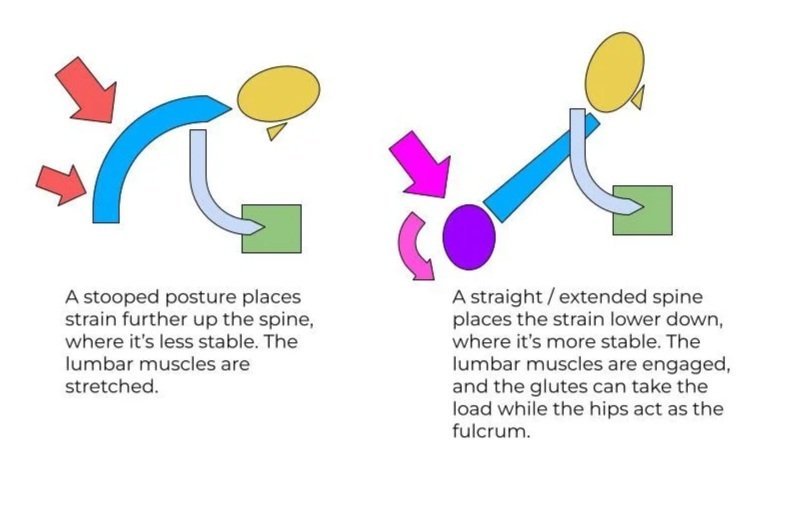
Fig 3. Although a very powerful group of muscles, the lumbar muscles such as the quadratus lumborum are best used for stabilising or bracing and the actual lifting done by the buttocks and hamstrings.
Strong Curves
The curvature of the spine also greatly increases its strength. The spine is attached to the pelvis at an angle known as the pelvic incidence, which varies from person to person. From here it curves forward - lordosis - then gently backwards - kyphosis at the thoracic spine. There is a further mild lordosis around the c-spine. Modern life tends to accentuate these curves, as in for example the ‘desk hunch’ (fig 4.)
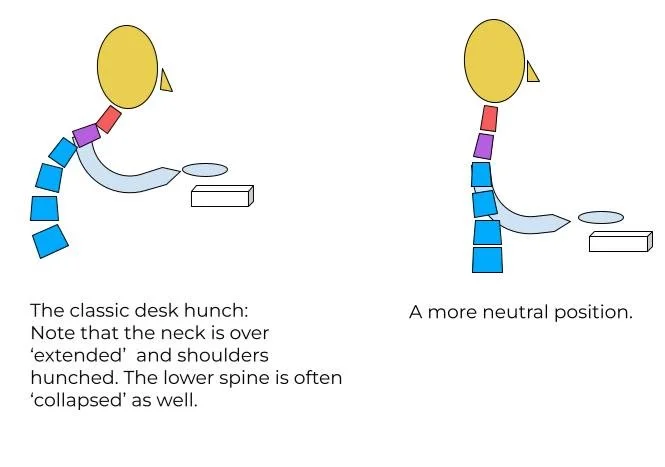
Fig 4. If you were to spend several hours a day looking up at the sky, it would hardly be surprising to develop pain in the neck and shoulder, yet this is effectively what we are doing while hunched over with our cervical spine ‘extended’.
As Behind, So At The Front
An exaggerated lumbar lordosis also, over time, shortens the lumbar muscles, making them less efficient and more prone to injury, such as the agonising spasm of the ‘locked back’. This progressive shortening and weakening of the lumbar muscles is one of the most common causes of low back pain. However simply stretching them out is only one half of the solution, because on the front side of the pelvis we also have the hip flexors which basically lift our legs up, such as when kicking a ball, walking, doing the can-can and so on.
Sitting for long periods also shortens the hip flexors, which has the effect of pulling the spine further into lordosis. While stretching and mobilising the lumbar muscles is important, it is a wasted effort if we are not also stretching out our hip flexors regularly.

Don’t neglect the flexors!
The 3 Column Problem
A final and less well known consequence of chronic hyper-lordosis of the lower spine is the effect it has on the facet joints. The spine has been described as having ‘three-columns’: We have the main body of the spine which are the vertebrae stacked over the other, but projecting from the back of these are the facet joints. These are also stacked one over the other in a complex configuration which I won’t even attempt to describe. All we need to know is that these also help stabilize the spine (and protect the spinal cord), and also help distribute the load. In the lower spine they take up to around 30% of the weight. (see fig 4.).
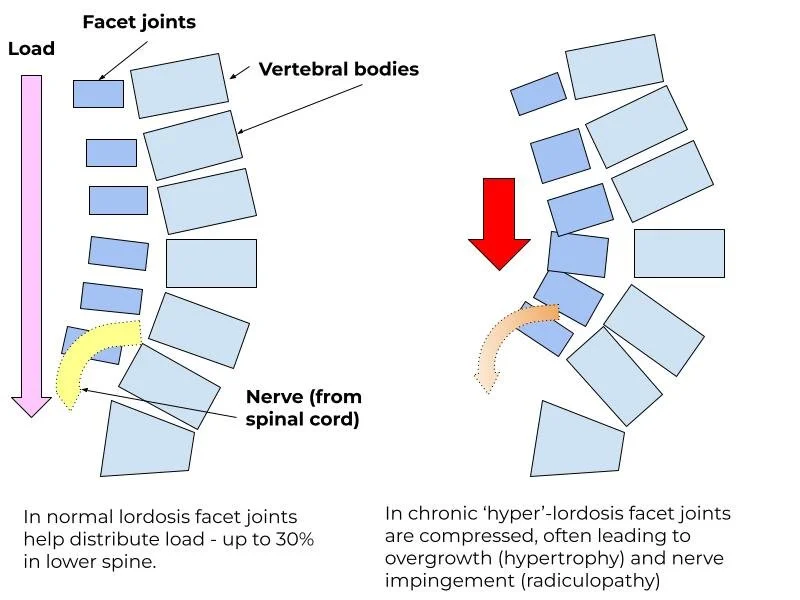
Fig 5. Chronic pressure on the facet joints, that project from the back of the vertebrae, can cause inflammation and hypertrophy, which in turn can touch or pinch the exiting nerve. (It is worth noting that there is no physiological reason why this can’t be reversed over time with the right alignment)
The Low Back System: Stocks, Flows and Feedback Loops
Looking at the low back as a system reveals why standard treatments - with the exception of physiotherapy - are often unsuccessful in the long term. However I wouldn’t want to give the impression that other treatments such as medications, injections and surgery etc. are not effective. They can be. Also certain surgeries, such a kyphoplasty play an invaluable role in returning patients to normal function. The following is simply to demonstrate that the most effective way to treat back pain is to return as soon as possible to normal activity. (see also box 3.)
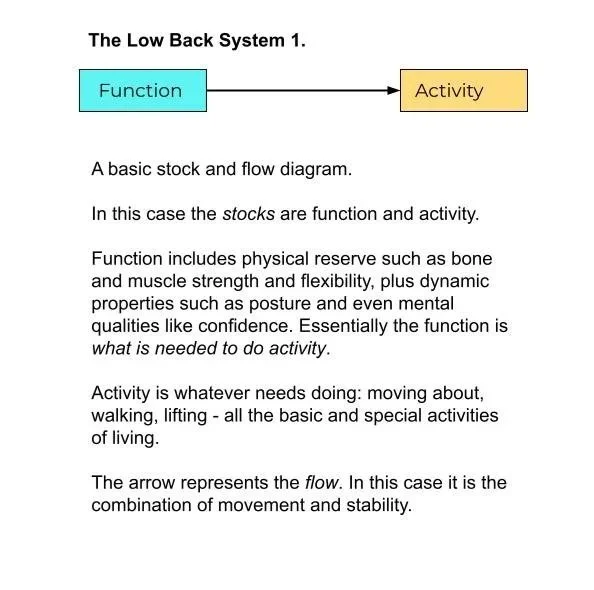
We can use a classic ‘stock and flow diagram to visualise the low back system in action.
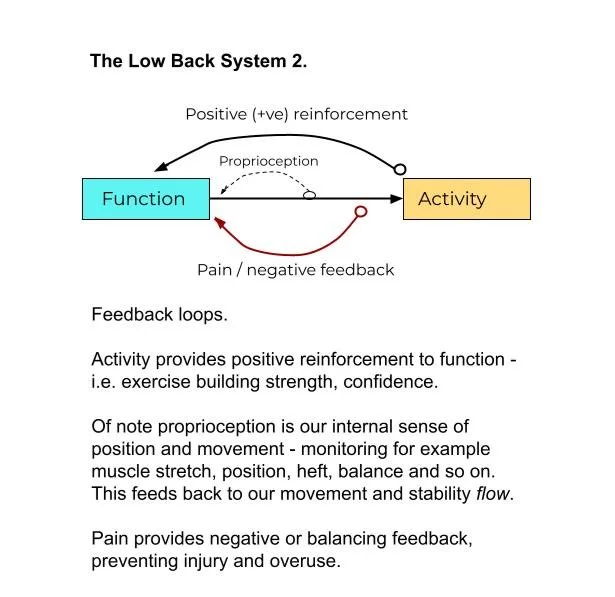
Most systems make use of feedback loops in order to maintain a stock at an optimal level. These might be reinforcing (e.g. virtuous circles or vicious cycles) or balancing (if too much then the flow is dialled down and vice versa. With the right kind of movement and activity, function is maintained, or even improved - a reinforcing loop.
Pain should act like a balancing loop, protecting the function of the back by inhibiting further injury while it heals. Even so, careful activity will continue to build and maintain function, ideally leading to a return to normal activity.
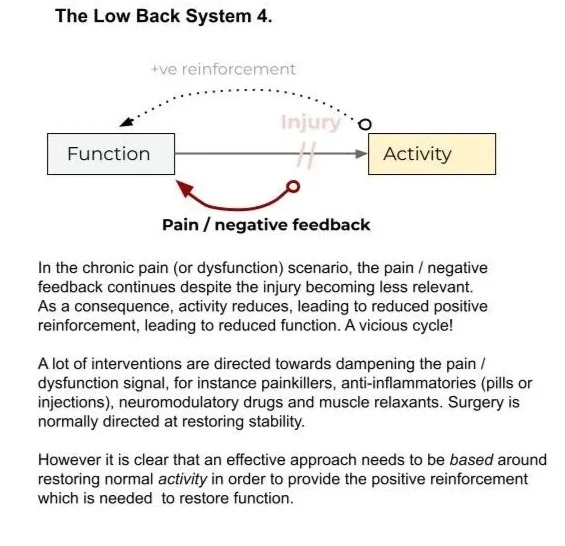
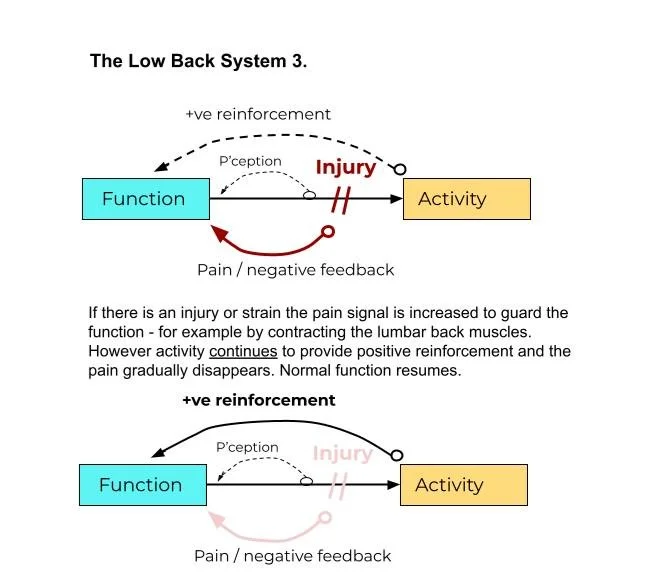
In the chronic scenario, pain shifts from being a balancing feedback loop to becoming a reinforcing feedback loop, leading to a loss of function, which in turn leads to more pain (it also affect proprioception). To make matters more difficult, activity decreases, no longer providing the beneficial reinforcing feedback to build function.
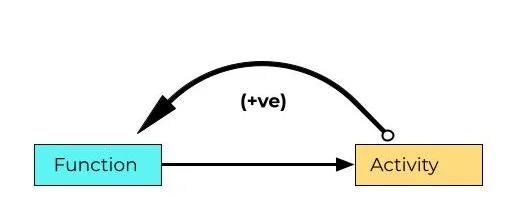
The ultimate aim of treatment is to restore the positive function → activity → function reinforcing loop. Perhaps the most important take home message is that chronic does not mean irreversible.
The Pelvic Tilt
The pelvis is a crucial component in the low back system. It is, if you like, the core of the core. The pelvis is, among other things; the base on which the spine is anchored and the fulcrum about which it pivots. The various forces from the upper to lower parts of the body are transmitted through the pelvis (including the various myofascial chains). To do justice to the pelvis is an article in itself, so for now we’ll just confine ourselves to one of its more basic mechanical variables - the ‘pelvic tilt’.
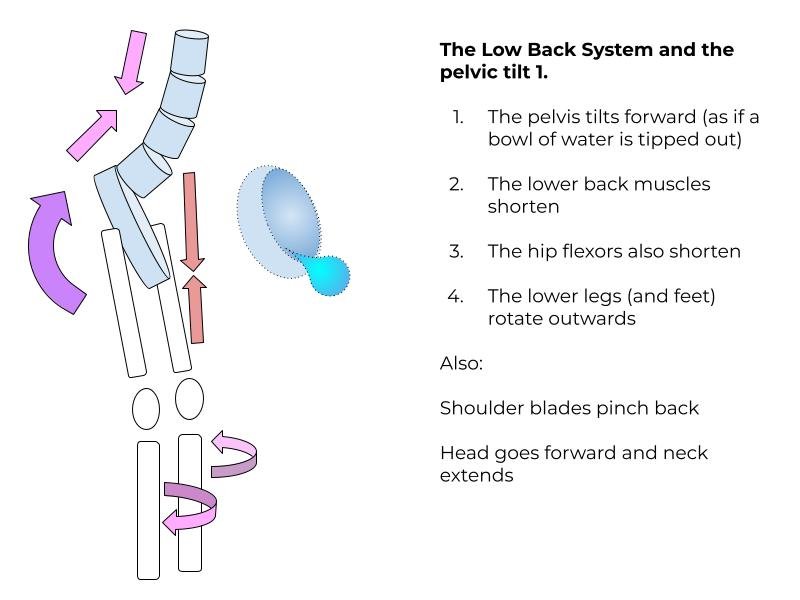
What is your pelvis doing at this moment? Is tilted back or tipped forward? If you are anything like me, it will be the latter, and I am always having to remind myself to tilt it back. If I am sat down, this means putting my weight on my ‘sit bones’ rather than the back of my thighs. When I do it affects - positively - every aspect of my posture, with a more erect head, lower shoulders and easier breathing.
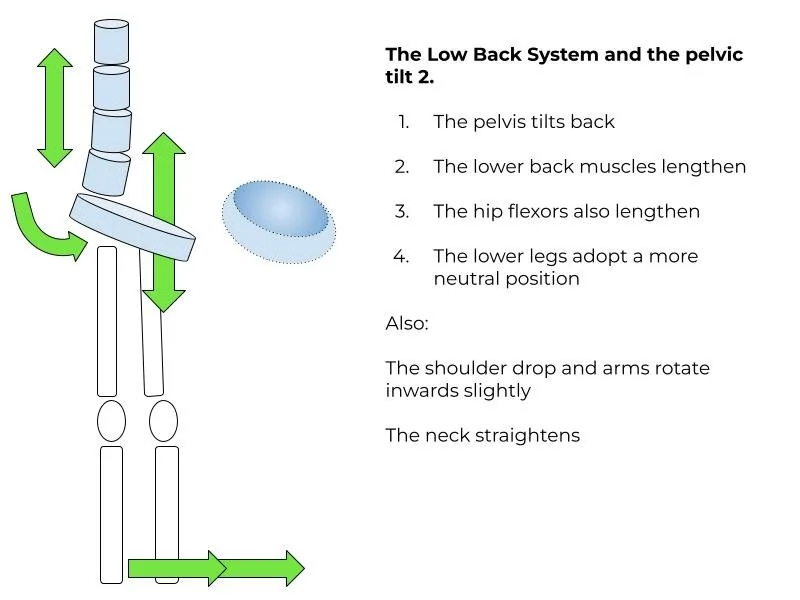
The benefits of tilting the pelvis back will be slightly different for everyone, but generally the flattening of the lumbar spine changes everything from position of the feet to the top of the head.
We are near the end of our low back journey. The principles of a well-functioning low back system essentially boil down to using our backs in the easiest and most efficient way possible - heavier work to the strong and stable parts, lighter work to the more mobile parts - and being mindful of when we might be putting strain where we shouldn’t.
These principles apply regardless of your age or level of fitness or activity. Pain is a signal that something has been pushed out of balance, but where we experience the pain may not correspond to the cause of the pain, and the ‘source’ of longstanding pain is often impossible to locate. Treatment of the pain often involves widening our attention to the entire low back system; from head to toe. In reality the low back system does not really have a beginning or end as it extends to include our work patterns, our beliefs about ourselves and so on.
Regardless of this, the best treatment for back pain can be summed up in a single word: activity: Activity reinforces function which improves activity and so on. The question naturally arises about what kind of activity, and for this we’ll keep it simple and say that experimentation is key. To move from trying to solve any given point and explore until you find something that seems to activate the system as a whole, and then keep going in small but consistent steps. It can take several weeks, or longer, but all I can say is that you’ll know when you’re on the right track.
Box 3. Back Pain Treatments - summary of the evidence
Exercise and activity including walking is crucial
In chronic pain small but consistent activity leads to increasing benefits
Psychological therapy can result in large and sustained effects
Medicine offer minimal benefit
Paracetamol (Tylenol) is no better than placebo
NSAIDs provide minimal pain relief and there are risks with long-term use
Opioids (codeine, etc) offer no benefit for acute LBP and little for long-term LBP
Muscle relaxants, gabapentinoids, steroids, cannabinoids show little to no benefit
Surgery and invasive procedure little to no benefit with most people w LBP
For older adults prioritise pharmacology and lifestyle (though with exceptions such as kyphoplasty for vertebral collapse fractures, as mentioned above)
Children and adolescents sport etc
Recent highlights in low back pain research, Part I: Diagnosis and Prognosis, Zambelli-Pinto et al. Journal of Physiotherapy, January 2026
https://www.sciencedirect.com/science/article/pii/S1836955325001456